
Argh. Cliff Asness is a true supervillain - he has succeeded in forcing me to think about health care. On Twitter, I repeated the factoid that America's health care system is worse than that of other advanced nations, and Cliff directed me to this article of his, alleging that this talking point is a myth. The whole article is too big to take on in one post, so I'll stick to looking exclusively at his "Myth #4":
Myth #4: Healthcare costs are very high in the United States compared to socialized countriesThis section itself is broken into multiple points, so let's take a look at them.
Many of the surveys of “outcomes” that show other countries spend less for similar or better healthcare than the United States are just intentionally disingenuous (i.e., they lie). The ultimate example is the U.N.’s 2000 World Health Report, which has been extensively cited by progressives and the media...[T]he study included high-speed auto fatalities and murders in their assessment of a country’s life expectancy, and then progressives cited that life expectancy to indict the U.S. healthcare system. Well, Americans drive more often on a more extensive highway system than most others, and we sadly have more crime than many. Reputable studies exclude these fatalities as, while tragic, they are not the fault of the healthcare system and should not be used to judge or modify the healthcare system. With these fatalities excluded, the U.S. ranks 1st in the world on life expectancy. With them included, we rank 19th, as reported in the 2000 study cited so often by ObamaCare advocates.Actually, with both violent fatalities (which include suicide) and traffic fatalities included, we rank 42nd. But anyway, Cliff's point is an important one. Still, I don't think he makes the case. Here's why.
First of all, this study, by Robert Ohsfeldt and John Schneider, uses data from 1980-1999; hence, it is between 34 and 15 years out of date. There is some evidence that the U.S. has fallen behind a bit since then. One way to see the old-ness of the study is to observe that the gap between the U.S. and the other rich countries was very small, with or without traffic and violent fatalities!
Read this WSJ article for a balanced look at the Ohsfeldt and Schneider study. Also, a quick Google will find some studies that look at more disaggregated metrics - for example, this 2012 study, which gives survival rates for various types of cancer. There are many, many other sources like this out there.
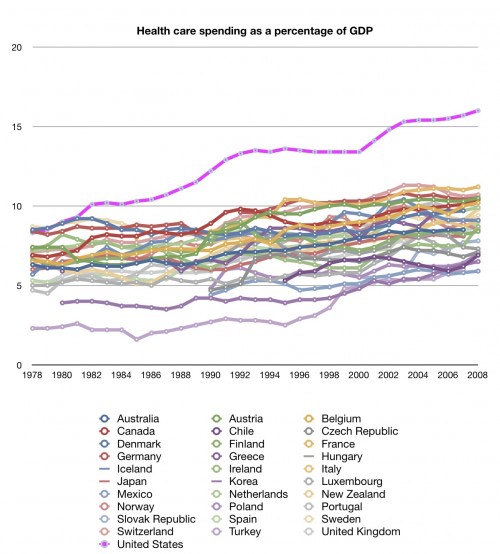
The upshot, though, is that in terms of life expectancy, and most other outcomes, the U.S. and European/Asian systems are doing about equally well. The U.S. simply spends a much much larger portion of its GDP to achieve this performance. Similar results for 1.5 or 2 times the price? That's a crap outcome, as a businessman like Cliff should know!
{kind=link}
Cliff also accuses the U.N. of basically lying to make the U.S. health system look bad:
Perhaps even more insidiously, most of the U.N.’s 2000 World Health Report does not really even rank healthcare outcomes. The actual oft-quoted final rankings, with the United States ranking poorly, are an average of many different ratings, many of them explicitly about how “socialized” or “progressive” a healthcare system is. For instance, their rating system gives 25 percent weight to “financial fairness,” and if one goes through their other categories you find they again are not rating who lives or dies or lives better (you know, healthcare outcomes), but how much the healthcare system has such things as “respect for persons” (this is part of the 12.5 percent weight they gave to “responsiveness,” which is separate from the 12.5 percent weight they gave to “responsiveness distribution,” whatever on Earth that is). The report goes further, judging these things with such objective measures as “respect for dignity” and “autonomy.” In total, more than 60 percent of a country’s score in this survey was some measure of progressive desires, not what you or I would call a healthcare outcome. And, as in our auto example above, much of the rest contained expressly anti-American flaws. That we pay for the United Nations to lie about us is a topic for another day.I don't have anything to say about this, but I never heard about those ratings anyway, and I don't think advocates of U.S. health reform really talk about them much. So I will skip over this part.
Cliff's later points address this somewhat, so let's proceed:
Part of the reason we spend more is other countries have price controls and we don’t. For instance, they restrict the amount drug companies can charge much more than we do. That sounds great; price controls save us money! But if nobody pays for new drugs, they don’t ever get created. Without these controls, our consumers here indeed pay more, but that funds much of the life-saving and life-extending healthcare innovation available for Americans and the rest of the world. It is frankly unfair that the world is free-riding off us. Free-riding means they let us pay for the innovation that benefits them at lower cost. But if nobody pays for the innovation, the innovation just does not happen. If we try to free-ride off ourselves, it doesn’t work—innovation dies for us too. U.S. consumers paying fair prices (not government restricted artificially low prices) does lead to higher U.S. healthcare costs, but the alternative is far worse: Joining the world in severely limiting prices, and not seeing the next generations of new innovations and improvements.This is another important point, though I wish Cliff had provided some evidence.
The U.S. spends 18% of GDP on health care; Germany spends 11%. Are you telling me that we spend 7% of our GDP - one trillion dollars a year - on health innovation? Actually, since some health innovation is done in other OECD countries, it's an even bolder claim - that $1T should represent the difference between what we spend on health innovation and what we would spend if we were able to "free ride" as much as Germany. That's a lot of health innovation spending. Health research spending is only about a tenth of that, actually. (Research is not the only type of innovation, of course, but it seems like the bulk of it, especially given that many R&D expenses are tax-deductible, so it's in companies' interest to classify as much innovation as "research" as possible.)
So the argument is that our exorbitant health care prices go to fund innovation, which Europe and Japan then get for cheap or free, by free-riding. But how does this free-riding work? How do they just take our technology?? Maybe ideas are just in the air, and technology spreads by casual conversation among doctors at international conferences, by cheap reverse-engineering, by industrial espionage, etc.
But if this is true, then health technology is non-rival and non-excludable - it's a public good! And a public good is a market failure. And if health technology is a giant, $1 trillion market failure, we shouldn't expect a free-market system to work very well. You can try to patch things with a patent system, but that will always be an incomplete solution. So if all this free-riding is going on, it's a powerful argument that much medical innovation should be done by the government, not by private companies.
Cliff continues:
Americans lead less healthy lifestyles than much of the developed world. Americans historically value freedom more than other countries and cultures. We value it for its own sake, even if it sometimes leads to a worse outcome. But we mostly value it because these choices are personal. Frankly, some would sacrifice some health to eat what they want and avoid the StairMaster. Freedom isn’t always sugar-free. Our American choices are costing us more, and raising the healthcare cost figures progressives love to cite. But they are our choices to make, not theirs to gainsay.I will spare the snarky comments about public health, hand-washing, sewer systems, the CDC, blah blah blah. Those comments write themselves.
What's less clear is that people in Europe and Japan are less free. Getting good health advice from your doctor isn't slavery. Being taught healthy habits in school isn't slavery. If you think either one of those things is slavery, you're a doofus. A doofus who is entitled to his doofus opinion, but a doofus nonetheless. (Note: This is a value judgment!)
(Actually in some ways we live healthier lifestyles than people in other countries. We smoke less, for example. Obesity is the main difference. It's a little amusing how the right has turned to extolling the virtues of land-whale-itude in recent decades...)
Cliff:
We spend more on end-of-life care than more regulated societies with socialized medicine or systems closer to it. That’s our choice.Is it? A lot of that higher spending is higher prices, which could reflect higher demand, or which could reflect inefficiencies in the system (or paying for innovation, but I covered that above). I'm going to go with "inefficiencies," since Americans usually don't even know the prices of the health care services they buy. How can you make an informed, free consumer choice when you don't even know the price of what you're buying?
Cliff:
The cost of a healthcare system is not just what we spend directly on it, it is also how much the healthcare system helps or hurts the overall economy. If socialized medicine slows economic growth, then this is part of its cost, perhaps a big part, and is left out of the simple analyses (looking at direct expenditure divided by GDP) that are so common.But if the government forbade us from spending money on health care, we'd just spend it on other stuff we like. In real terms, if government forbade us from using real resources to create health care services, we'd use those resources on something else we want a bit less. Substitution would mitigate the effect of price controls, etc., not exacerbate them.
Cliff:
Lawyers. We got lots, they have far fewer. We can separately debate how to design our legal system (some of my libertarian friends advocate for a large role for lawyers), but the size and scope of legal action here dwarfs most of the world. It leads to doctors practicing tremendous amounts of “defensive medicine.”This is a sensible point, but as with most of these points, it's not backed up by any numbers or evidence. Tort reform could theoretically be a big money-saver, but in practice it doesn't look like a game-changer.
This brings us to the end of Cliff's so-called "Myth #4". The main take-away is:
1. We pay much much more than other countries for about the same quality of health care.
2. Some part of this may be due to innovation externalities, but these must necessarily represent a market failure.
Anyway, I do think Cliff's points are important. I think medical innovation is very important and under-studied, and I do think it represents some (though not most) of the price difference between America and other countries. I do think that tort reform is a good idea and should be tried. I do think that the difference between America and the rest of the OECD is not in health outcomes, it's in the cost we pay to achieve those outcomes. And I do think that the medical system can't entirely fix the obesity problem.
But these points do not convince me that the American health system is doing better than those of other rich countries. Cliff's main point is that the American quasi-market system, while not perfect, does many things better than the non-market systems of places like Germany, the UK, or Japan. But it seems to me that getting "bang for the buck" for the modal or median person is not one of these things. Cliff's "Myth #4" seems like no myth, but fact.
A quickie response to getting your ass kicked on twitter.
ReplyDeleteBut my abrupt silence on Twitter was due to the fact that I started writing this post...
Delete:( Tenure track doesn't follow nonsense like this, arkboy
Deleteand thus....x ....the remaining is for free...to frame him fitting shape and strange
DeleteUS of A great and grateful sacrifice
Lies cauld in her grave, and will never return....
The US has deliberately created healthcare monopolies with huge pricing power and little competitive accountability. The fact that it's a much more rural country makes this worse:
ReplyDeletehttp://www.nationalreview.com/agenda/385283/threat-health-care-market-consolidation-reihan-salam
Tort reform, for the most part, means that injured people don't get fully compensated for the harms that they suffered. If you're talking about the tort reform which prevents meritless lawsuits from ever being filed, you're off in conservative-fantasy land.
ReplyDelete(Also, how do you know medical innovation is under-studied? Is it under-studied by the medical community at large, or Megan McArdle, or you?)
Funny how the seemingly endless comparisons of the US healthcare system to other countries don't carry over to the respective legal systems.
DeleteIn the US, settling frivolous lawsuits for tens of thousands of dollars is often, pathetically, the right business decision. The simple system of 'loser pays,' which most other developed nations employ, never merits a mention in the major media.
US has loser pays too. When you get sued, you slap them back with a counter-suit that includes the court costs and lawyers fees.
DeleteProblem is that even with "loser pays," if court rulings are not always 100% correct, you can end up paying boatloads in legal expenses, on average.
Um, we're talking about an estimated 2.4% of health care spending (for legal expenses, insurance, defensive medicine, etc., according to a 2010 Harvard School of Public Health study). And some part of that is to provide compensation to people who have been at the raw end of some real malpractice, so 2.4% is the absolute high end of the cost "frivolous lawsuits" impose on the health care system.
DeleteContrary to conservative myth, lawsuits are hard to file and hard to win in the US. You need a professional lawyer, so lots of people with real damages don't get compensated. And making *all* cases harder to file (as proposed reforms usually go) doesn't do anything to separate the frivolous and the real cases.
Of course, part of the myth is that all lawsuits are frivolous. A doctor, who's likely part of the top 1%, left a scalpal inside the waitress he operated on? She has no insurance so she needs money to get it removed? How dare that peasant beg for money from her social betters! Clearly the suit is frivolous! Does she have a medical degree saying that she knows she shouldn't have scalpals in her? I think not!
Also, I can't even think about the frivolous lawsuits argument without remembering that scene from A Tale of Two Cities where the Marquis runs over a peasant kid with his carriage, throws a coin at the father, and then becomes angry when the father isn't properly grateful.
DeleteDickens is one of the few writers who recognized these people for what they were.
The nice thing about Noah's blogging is that he makes no effort to hide his total ignorance. Most economists simply hide their ignorance about the legal system in their assumptions.
DeleteResearch and development is actually only about 2% of US health spending. CMS says it's a pretty measly $50 billion: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/downloads/proj2012.pdf
ReplyDeleteI don't know what the actual difference in R&D is between the US and the other countries, but show me the math where $1 trillion can be the difference between two positive numbers less than $50 billion.
I don't follow your argument that health innovation is a public good. Suppose a pharmaceutical company invests in producing new medications because Americans pay a lot for them. Once the medications are developed, the pharmaceutical company might as well sell them at marginal cost to non-Americans (given that any higher price is not allowed) as long as there is no fear of arbitrage. The argument is not about stealing technology or non-rivalrous or non-excludable medications.
ReplyDeleteHealth innovation is a public good because "intellectual property" in general is a public good, a fact that most (though not all, thinking of some libertarian schools) capitalists try very hard to obscure.
DeleteBy definition, ideas are non-rivalrous. The Platonic Form of a circle does not gain sharp edges if more people become aware of it. And though governments throughout history have tried very hard to keep ideas away from people at the barrel of a gun, they all fail sooner or later. At most, health innovation can be a delayed public good, while the ideas inevitably seep out into the public domain (and into the manufacturing plants of Indian generic drug makers).
MDZX
So what? Why not respond to what Joshua Weiss wrote instead of going off on a tangent.
DeleteSure, Noah interpreted one of Cliff's arguments in some fashion, but Johsua reframes Cliff's argument the way it was intended to be interpreted. Now, preferably without invoking Plato, how does Noah's argument apply to what Cliff was actually arguing?
or Cu its not it's the same ....hit's and hitmen.....
Deletewithout invoking Plato under Socrates cock?
I think it's better to compare specifically to the UK than to Europe in general, Japan, etc. To a first order approximation, the UK is identical to the USA in practically all relevant demographics (poverty, race, obesity, rural/urban mix, etc)*. Yet, public health expenditures alone in the US are much higher than total health expenditures in the UK. Add in private expenditures and the US spends over twice what the UK spends per capita for the same outcomes (you can cherry pick either way to say one or the other is better). It's obvious that, ignoring political and legal barriers, the US could nationalize healthcare exactly following the blueprint of the NHS and solve the medium/long-term budget gap and lack of health insurance for several million people without negatively impacting anyone except those who profit off American healthcare inefficiency relative to other nations.
ReplyDeleteRepublicans shouldn't be allowed to treat the national debt as an existential crisis (though only when Democrats are in power) and then nitpick the relatively tiny problems in the NHS as a reason why nationalized healthcare is impossible.
* A little more complicated if you're including crime and suicide on account of guns
One reason the UK system developed the way it did was because during WWII the government took over all the hospitals. They basically had to; otherwise, how were the casualties from the Blitz going to be paid for? So by the end of the war, the UK already had the basis of single-payer in place. The U.S., on the other hand, because of price controls, had evolved a Rube Goldberg system of employers paying for health insurance for their employees because they couldn't give them pay raises. After the war the U.S. didn't have a big incentive to change that, and the insurance companies had a big incentive to fight any change. They still do, which is why we won't be able to adopt single-payer for at least another fifty years. Even if The Oligarchy hasn't formally come out and taken over the government.
DeleteNoah, your argument about patentable healthcare R&D being non-rival and non-excludable has persuaded me that there is no such thing as private sector innovation, since by definition any such innovation becomes a public good if somebody copycats it. Hence, all R&D should be funded by government, healthcare or otherwise. I'm sold.
ReplyDeleteThe importance of your convictions might be improved if you weren't a consistent doofus.
DeleteProject much?
DeleteThank you for acknowledging my consistency.
DeleteFinding healthcare data that actually is comparable is a chore. Nevertheless, I think it's pretty apparent that the (old) US system is a poor system.
ReplyDeleteHowever, in regards to us funding the development of drugs for the entire world, I think your response is not very good. I'm not sure what the law is, but I believe that even German drug companies are charging Americans more for their drugs, as the same laws and institutions that allow drugs from US drug companies to be expensive in the US apply to German drug companies as well.
In this sense it is possible (though I DO NOT have any evidence of this) that drug companies world-wide are depending on US drug sales to fund their research. In which case changing the US system to single-payer with the enhanced bargaining abilities would decrease drug R&D worldwide and, conversely, getting rid of other single-payer systems would decrease US drug prices.
While I do think that the bigger prices we pay for drugs are A reason the US system is more expensive and that less single-payer systems world-wide would bring down US costs, I do not think it is the root cause. It is also worth noting that the US has no responsibility to fund drug research the world over, and that other countries aren't likely to change their policies. So, even if it means less drug R&D we should probably move towards a single-payer (or at least single-drug-price-negotiator system) especially since in the long run if their is no new drug research countries are more likely to work together to fund new drug research if they don't have the option of just letting the US pay out the nose.
Don't think so. See my comment above. In footnote, CMS says they counted R&D for drugs under research, so that is in the $50 billion total US spending on health R&D. Still orders of magnitude away from explaining difference in cost.
DeletePut another way, only about 14% of drug costs are R&D, which is nowhere near the size of the gap between US and European healthcosts.
Dean Baker returns to this frequently. He points out that there are other ways than government-granted monopoly pricing (patents) to fund R&D. After all, the National Institutes of Health pay for a lot already, which Big Pharma happily makes use of. The government-granted and -enforced monopolies inevitably lead to a lot of corruption.
DeleteSo we move from #1 to #41 if you include traffic accidents and acts of violence ?
ReplyDeleteAm I the only one that finds that more scary ? Are we possibly worrying about the wrong things ?
Perhas, but different issues.
DeleteYes, but if its true that despite the best health care we end up dying younger due to traffic accidents and violence (where we're presumably well past #41 on this list ) - shouldn't we be looking at curbing those things ahead of fixing healthcare (where we're #1)
DeleteThe difference in life expectancy between the US and Sweden is 3 years in Swedens favor. In a population of 310 million, how many 18-year olds must perish each year to lower the life expectancy 3 years?
DeleteThe maths is not hard. The answer, incidentally is higher than the number of soldiers the US lost in WW2. Which is part of the reason that study that blamed car accdents and violence for differences in lifespan were ridiculed.
How dare you question my Constitutional right to own an AK-47 and drive an SUV at 65mph in front of schools! Communist!
Deletehow many 18-year olds must perish each year to lower the life expectancy 3 years?
DeleteMost of them are just blacks, Hispanics or trailer trash - so they don't really count. :-)
Yes, well. My point was that simple maths show that the number of deaths necessary to drop average life expectancy by 3 years is absurdly high. So high it should be obvious that car accidents and violence can't be the cause.
Delete(The health care systems speed of response and quality of treatment should significantly affect the number of car and violence incidents that turn into fatalities)
It's not scary because it's not true. That Cliff person, whoever he is, is bad at arithmetic.
DeleteSimple question: how does one compute life expectancy while excluding some sources of fatality? Is it based on the assumption that homicide victims (for instance) would have had health outcomes matching those of the rest of the population on average had they not been killed? Doesn't this replace one source of bias with another?
ReplyDeleteThat's effectively what they're assuming.
DeleteThey're also assuming that people who get hit by cars or are the victims of homicide/suicide are just as likely to die in every country. Most people who get hit by cars don't die, and who knows if the US is particularly bad at saving people who were in car collisions.
More or less like this -- it's not perfect because of definitions of "at birth" (people who die in car crashes this year were born in earlier years, for example) but it's close-ish:
Deletehttp://dr2chase.wordpress.com/2012/12/13/democrat-math/
I'm not sure what bias you're expecting to see, either. The computation I use simply excludes the murder/crash deaths and computes the life expectancy of the rest. In a counterfactual if-those-people-weren't-killed, if those people are just like the rest, then the counterfactual-expectancy is the same as the excluded-expectancy. If they instead die sooner than average (perhaps because car crash deaths are associated with poor choices which might generalize to other causes of early death), then counterfactual-expectancy would be *lower* than excluded expectancy.
Only in a world where the crash and murder victims would have lived longer than their peers do we see life expectancy exceeding the excluded-victims-estimate if we assume that crash and murder deaths are avoided.
The media, and the public at large, also has a tendency to exaggerate small (but catastrophic) risks, while downplaying substantial (but less "sexy") risks. That helps explain our national obsession with terrorism, even though you are much likelier to die in a car accident. And as scary as mass shootings are, you are more than twice as likely to die from suicide (12.4 deaths per 100,000) than homicide (5.3 deaths per 100,000). (Gun homicides cause 3.6 deaths per 100,000.)
ReplyDeleteSuicide is actually the #10 leading cause of death in the U.S. (See chart.)
Noah, Maybe I am in a liberal bubble, but everything I have read says the effects of lawsuits on healthcare costs are minimal.
ReplyDeleteWhat angel are you looking at ?
Bill, I don't know the answer, but he assumes other countries don't have lawyers. The NHS in the UK pays £billions in negligence claims. I have no idea how it compares the US, but it's not trivial.
DeleteIn fact, studies show that in the USA there's far, far more money left on the table in unpursued, legitimate malpractice claims than rewarded to illegitimate claimants and their lawyers. Truly "fair" malpractice reform would both identify those who are injured without compensation and identify fraudulent claims; this would increase the costs of healthcare and malpractice insurance, but would reduce negligence rates.
DeleteI love that Asness ran off into "deluded rich guy" territory near the end there. Americans historically value freedom more than other countries and cultures. We value it for its own sake, even if it sometimes leads to a worse outcome.
ReplyDeleteGot any real proof for that, Asness? Because as far as I can tell Americans love "abridgements of freedom" when we benefit from it. We've had an explosion in occupational licensing, Medicare/Medicaid/Tricare are all quite popular even if people have a few criticisms, and so forth.
We spend more on end-of-life care than more regulated societies with socialized medicine or systems closer to it. That’s our choice.
This is a regurgitation of a very old anti-universal health care point I heard once, about how the US was so magnanimous that it put the people who had good insurance in wheel chairs while the poor had to hobble around on canes in "bad old Europe".
Anyway, I do think Cliff's points are important.
Not for the reason you think they are. They're a laundry list of conservative bullet points about health care that they have little proof for but basically dredge up every so often whenever progressives are in a position to make progress on health care reform.
That freedom silliness reminds me when I was in 4th grade and a Swiss woman came to talk to my school about Switzerland, and someone asked her if she felt more free in the US.
DeleteContrary to popular opinion, Europe is not just gulags, fascists, and smelly cheese.
Here's a question I asked in 2010 about how our healthcare system could be better, or at least worth it:
ReplyDeleteWe spend about $100 billion per year on medical research, public and private combined (see here).
We spend about $2 trillion per year on health care delivery, the doctors, hospitals, administration, etc. If we adopted a European style system, cutting our spending per person in half, as in European countries (that I think the evidence shows have about as good or better health care and results anyway; see for example here), then we would save about $1 trillion per year.
Now, what if we spent that $1 trillion in savings on medical research? It would increase medical research spending more than 10 fold.
Even if delivery did get a little worse, even if we did get a little bit less of our brightest and best becoming doctors due to lower pay, it seems like this would be totally outweighed over the long run by tremendously more advanced medical understanding and treatments due to the 10 fold increase in medical research spending (or more, as some advanced universal healthcare countries provide comparable health care to the US at about a quarter of the cost per person) .
So it looks like if you want better medical results, better treatment, breakthroughs in rejuvenation, better odds of surviving cancer, you name it, you should support going to a European style system, and using the immense savings to increase medical research more than 10 fold.
So if our health care system really is more efficient than the Europeans, then why is it possible to make such a vastly favorable trade?
If the Republicans really care about our children and grandchildren so much why don't they do this, so in 50 years they could have medicine as advanced as it would take perhaps 150 years to achieve with our current system. I don't care how bad you imagine European health care to be, you cannot think a European medical center of today is less effective than even the Mayo Clinic of 100 years ago, when penicillin and polio vaccines hadn't even been invented.
at: http://richardhserlin.blogspot.com/2010/01/if-our-health-care-system-really-is.html
The entire worlds biomedical research budget is 248 billion. It could be quadrupled.
DeleteSeriously, though, not only does no one ever answer this question, but no one ever asks it!
DeleteReally, I feel like this guy:
https://www.youtube.com/watch?v=wC8y0HoopVE
if we exclude December, January, February, March and April, Minneapolis has a great climate
ReplyDeleteYou brushed over what's actually the most important point.
ReplyDelete"We spend more on end-of-life care than more regulated societies with socialized medicine or systems closer to it. That’s our choice."
It's actually not "our choice" in the sense Cliff means it of personal, private spending decisions. At least 90% of it is Medicare. It turns out that a huge part of the reason Americans spend so much more on healthcare than Canadians and Europeans is that one of the parts of healthcare that we mostly socialized, care for people in their final six months of life, is extremely more spendy than in Canada or Europe. Our variety of socialized medicine simply has no spending control.
I'm not saying the greater obesity or the private vs public mainstream healthcare don't matter, but they're actually a relatively small part of the explanation of why Americans spend so much more. It is mainly in the last six months of life.
Yes, and so many of us would rather not have "the system" impose these end of life heroic interventions upon us, but "the system" finds it's bread buttered here and so on it goes...
DeleteSorry about the typo should be "its" not "it's". Doh! I knew that.
DeleteWell, nobody likes the idea of "death committees", but somehow in Europe, Canada, Japan they managed to implement them without great fuss. I see two reasons we went another way: we were significantly wealthier than they back in the 60s-70s when these political/cultural patterns were set, and our socialized Medicine is publicly funded but privately delivered, so there's a big, powerful lobby that kicks back plenty to Congress and the parties defending all-out spending for the terminally ill.
DeleteUh, UK,Germany and Japan all have parts of a "market system" into their national systems. All countries have national systems including the US. US costs rocketed between 2002-2008 because of monopolization of industry.
ReplyDeleteCliff sounds like he wants a global market system so capital owners can decide what "health care" I get to choose from and how I want it through some pricing scam.
Never trust merchants with finances. They would sell earth down the drain and join a invading alien force if they could make some profit.
There are two types of innovation. Innovation that is costly and innovation that is cost saving. The problem with putting the entire emphasis on costly innovation, is it deprives us of saving innovation.
ReplyDeleteHasn't Dean Baker been banging on about this for literally over a decade?
ReplyDelete1) Guilds like the AMA in the US keep the supply of doctors too low, and therefore their wages too high, relative to the rest of the world, and
2) The US patent system is basically a giveaway to Big Pharma that creates vast amounts of waste and corruption (incentives to cheat and misrepresent research as well as spend money on clones of successful drugs in lieu of spending on new ones go up a lot when strong patent defences are in play) that could be sensibly overhauled by either increasing the already huge chunk of R&D that government pays for and letting the free market simply manufacture drugs, as is done in places like India where you can save 90-99% on drug costs, OR setting up some sort of a Stiglitz prize system where companies compete for a government cash prize, with the resulting drug released to the free market for manufacturing.
MDZX
What about health inequality? Health care is available to everyone in a socialized health care system like in Europe, but not in a privatized system like in the US. So on average health outcomes may be comparable, for many people it most definitely isn't. And I think that is a very important distinction. The big relative gains for the American rich in health outcomes don't weigh up against the truly crappy health care available to the poor. So I really don't think that outcomes are comparable.
ReplyDeleteCliff says he doesn't even know what the argument you're making is about. Poor people deserves health care? That's unpossible!
DeleteIt's not that the poor don't deserve healthcare. It's that they are freely choosing not to get it by making the conscious choice to be poor. Why do you hate our freedom?
DeleteIf you start focusing on the variables that lead to treatment/hospital visits, the whole exercise in comparing health systems just becomes a waste of time. Nearly 30,000 people commit suicide in Japan per year. It's the #1 killer of young men. I'm pretty sure (no stats) that there's a pretty large number of those who get rushed to the hospital and receive some kind of (potentially costly) treatment before they die. Not to mention the number who don't die and end up receiving ongoing medical treatment. The idea that we should just erase these numbers (and car accidents and gun injuries from the US numbers) from the overall stats because they are inflated compared to another country is just flat out stupid. Every country has it's own specific risk factors for its citizens needing to access medical care. When Asness strips out just the stats he wants from the US figures, he's being much more disingenuous than the people he's accusing. What a schmuck.
ReplyDeleteA few points, if I may. The US spends 18 % of GDP on healthcare, where other nations spend 9 %. The difference constitutes what is normally known as "a godawful" amount of money. The entire military budget is 5 % of GDP.
ReplyDeleteWhere the money goes has actually been looked at very, very seriously. Health Affairs have had some articles about it.
From memory, about 35 % of the waste is excessive bureaucracy and administration. 35 % is inefficiency and over provision. 2 % is tort and 9 % is defensive medicine. 11 % is higher salaries, and 6 % higher drug costs. The remaining are small items.
I recommend those who are interested google the articles and read them. Its twice the military budget wasted every year, and we do know where it goes. No need to guess.
Second, on the subject of how america measures up to other nations healthcare systems, there are a number of ways to measure the performance of a healthcare system. When we do, large, overarching measures are chosen, to even out confounding factors resulting from special conditions relative to the country measured.
You can look at maternal mortality, average lifespan, infant mortality, number of years lost to ill health, amendable mortality, number of years lived in good health etc. The interesting thing is that the US places roughly the same for all those. Out of just over 40 developed countries, the US is mid-thirties on most of those. Mid fifties for infant morality, and high twenties for average lifespan.
So US results cluster fairly predicatively in the mid-thirties.
Hmmm... Out of just over 40 developed countries, the U.S. places in the mid fifties... ;-)
Deleteso,medical innovation is very important for health care. then U.S Spending 18% of GDP for health care..:)
ReplyDeleteWe need to make mention of the anxiety differential, also. In the US, one broken leg could wipe out a decade of family savings, or would have before the ACA. A senior, going into a nursing home under Extended Care (because Medicare does not cover long term care) immediately loses their home and savings, due to pay-down requirements of entry into that program -- no inheritance for their family, and no financial leverage to ever allow them to leave the care home, either.
ReplyDeleteEven for people who had good insurance, pre-ACA, you could never be certain whether it would be there when you really needed it.
The difference in mood, in fear versus comfort, in economic jeopardy not just for the sick person but for their entire family, can't be over stressed. To pay double for the same care, and on top of it have this corrosive anxiety ... there's no word for how stupid that is.
Noni
Noni:
DeleteVery true. It would be kind of you to answer over on my thread to a particular person who disputes the TN expansion of Medicaid.
US consumes extraordinary amount of painkillers because for too many people this is such a shitty country to live in. do we adjust for that too ?
ReplyDeleteGreat article! Perhaps you are too kind to Cliff though. Take a look at inexpensive generic drugs taken off the market, re-purposed as "orphan drugs", then sold at ludicrous markups: ACTH and GHB are two examples. As Jim Kunstler put it, the problem isn't capitalism, it's racketeering.
ReplyDeleteDenmark, where working after 5pm is grounds for insanity, for instance reports very high "happiness". No wonder they don't have to spend so much on healthcare as the miserable denizens of violent depressed soul-sucking America. If we adjust for the blatant inequity of other countries being less miserable, I'll bet US comes out top for healthcare
ReplyDeleteThings are improving, US's labour force participation rate is collapsing
DeleteNot every issue is measurable in life expectancy. The USA has about 1.3 million personal bankruptcies per year. It is estimated that 50-60% are due to medical bills. Let's say half a million families go bankrupt annually. That is an enormous amount of human suffering. Do other nations have this problem?
ReplyDeleteMany of these underinsured are not in a position to improve their situation by cooking meth. I do wonder if significant numbers do turn to the black market or criminal enterprises to live.
The innovation argument is weaker than you suggest. A great deal of medical and pharmaceutical research is done by the public sector -- NIH and others -- which can be and is commercialized by drug companies. Also, drug companies are notorious for concentrating research on areas where profitability will be highest, or on "me too" drugs, whether or not these criteria coincide with the public interest. Not to mention the very large sums (as much as R & D?) spent on advertising and promotion.
ReplyDeleteIt does seem that there could be big social opportunities for more public investment into research into cost effective treatments and cures for diseases that don't offer a lot of profit potential.
ReplyDeleteI don't understand the appeal to the free market by defenders of the status quo. Healthcare is a very heavily regulated market. You and I can not start a hospital, medical school, or insurance company without encountering thousands of laws, rules, and regulations imposed by federal law, state law, or professional accrediting rules. For example, the pot of medicare money is divvied up by a AMA organization, the RUC, which is a small group of specialists for the most part. There are lots of other examples; imagine starting the Discount Drive-In Abortion Clinic in a high single mother area.
ReplyDeleteOther nations have laws and rules that shape their system. We have our laws and rules, too.
Mr. Smith:
ReplyDeleteI would not waste your time pursuing Malpractice Reform as many states have already capped jury awards at $250,000 to $500,000. "Attorneys will not take a case unless they can win and make a living. The investment of $50,000 to $100,000 by an attorney to litigate a malpractice case presents a high economic hurdle." http://angrybearblog.com/2014/01/why-attorneys-will-not-always-sue-in-malpractice.html#sthash.8JRKB5o9.dpuf
“The health care system looks like a giant lottery. That is what it looks like these days with these lawsuits and somehow the trial lawyers are always holding the winning ticket.” In reality, far more people do not get their day in court to rectify a wrong done upon them through accident or negligence by doctors, hospitals, or the industry. Attorneys are the gatekeepers to whether a plaintiff receives their day in court. Before taking a case, “personal injury lawyers in both reform and non-reform states take into consideration the same three factors;
• the monetary value of the injury (damages);
• the factual components of the case, including their assessment of their ability to demonstrate wrongdoing or negligence on the part of a doctor or product manufacturer;
• their estimation of how the potential client will be evaluated by a jury (“likeability”).
This is a clipping of an article I wrote at Angry Bear Blog earlier this year revising what I had written previously. If we wished to resolve many of the issues with lawsuits, I would look to malpracticing doctors who are not policed by the AMA. Public Citizen has a nice article on it. "The Great Malpractice Hoax" http://www.citizen.org/documents/NPDB%20Report_Final.pdf
Hard to tell which healthcare system is best.
ReplyDeleteHard to tell what makes the best systems so good and what makes the bad ones so bad.
Hard to define what a good healthcare system even is.
Hard to disentangle the effects of the helthcare system on health outcomes from environmental and other exogenous factors.
Hard to convince everyone that the system needs to be chamged this way rather than another way.
Hard to actually change it even if you get everything else right.
And if you manage to change it, how long until theres pressure to change it again?
The world is too complicated.
I had an interesting conversation with a drug company lobbyist not long ago. The topic of the high prices of patented drugs came up. He went into the usual "innovation line." I countered with the fact that drug discovery is largely publicly funded (here and abroad). He conceded that point but then went on to highlight the expense (and time) involved in obtaining regulatory approvals.
ReplyDeleteAnd that's where that trillion goes. To expensive regulatory processes, some of which are unique to selling in the U.S. market (so much for a public good).
But somehow, the "conservative" health care talking points don't really focus on this point at all. It's probably because they love big, inefficient, government or something.
Don't forget that there's a history here. Historically, the original question was why health care in the U.S. was so expensive. There's been a lot of shilly-shallying, everything from the U.S. rulez innovation to bad outcomes for certain subgroups pulling down the average. But it's all been a dodge to avoid the original question of why costs are so out of line. This is important because costs are directly observable phenomena; everything else has been temporizing in the style of Kipling's just so stories.
ReplyDeleteThe claim about homicides and suicides comes from Schneider and Ohsfeldt's book, meaning it comes from the AEI. It is wrong.
ReplyDeletehttp://theincidentaleconomist.com/wordpress/this-stuff-about-life-expectancy-is-old-news/
In addition to what Carroll shows, most people don't realize that early deaths from the combination of homicides, suicides and accidents occur more often in rural areas than in urban ones. Most people worry about homicides in cities when accidental deaths are more frequent. Part of the reason for that higher death rate is the lack of medical care in poor, rural areas. (Disclosure, I work in multiple trauma facilities, including a poor rural one.)
On malpractice, of the estimated $50 billion from malpractice, most of that is from estimates of defensive medicine. When you look at states that have passed aggressive malpractice reform, Texas of instance, costs have not gone down.
http://theincidentaleconomist.com/wordpress/meme-busting-tort-reform-cost-control-2/
All that said, your point about ROI is spot on. For the amount of money we spend, we get a lousy return.
Steve
"But if this is true, then health technology is non-rival and non-excludable - it's a public good! And a public good is a market failure. And if health technology is a giant, $1 trillion market failure, we shouldn't expect a free-market system to work very well."
ReplyDeleteYou seem to feel like Cliff's argument fails to account for the public good nature of healthcare innovation, but I'm not sure you're correct. The reality of the US healthcare system is that there are huge public subsidies - both in the form of direct government spending on healthcare, and tax incentives for private spending.
Consider roads for instance - a classic public good. Imagine if instead of having the government pay for roads, we had private enterprise build them instead. Owners of roads would then be allowed to charge for their use. Normally, this would result in huge deadweight losses as private road owners would charge significantly more than the marginal cost of driving on the roads. Now imagine that the government stepped in to provide direct spending and tax incentives to foot the cost of road construction, while at the same time encouraging a system where the marginal price to use the road was fairly low (equivalent to a copay in insurance terms). The government also put in place cost controls to ensure that it didn't spend too much for people to use the roads.
Such a system would ensure that the marginal cost of using a road was fairly low, reducing deadweight losses from people changing their behavior. It would also make roads profitable to build in cases where the marginal cost of a road might be below the average cost.
Such a system, which is analogous to our healthcare system, largely accounts for the economic particulars of public good provision, and I think that may be Cliff's point. Cliff's doesn't dispute that healthcare is a public good, and that absent government intervention there would be a market failure. Cliff is merely pointing out that by paying prices for drugs above what could be negotiated, the government is effectively recognizing the public good nature of health care and dealing with it in an appropriate way.
This is not to say that there aren't problems with the specifics of how the government pays for drugs, or other parts of Cliff's argument (there are). I'm merely pointing out the notion of healthcare as a public good subject to market failure is completely consistent with Cliff's argument about how the US subsidizes drug development by paying higher prices.
Noah,
ReplyDeleteI know one could say this about a lot of things, but check out Paul Krugman's wirtings on healthcare...
-Libertarians may hate this, but the biggest drivers of increased life expectancy are the most socialized forms of medicine-vaccines and public sanitation. And tragically, as a society, we are turning on them, rejecting vaccine science and allowing public sanitation systems to rot.
-Libertarian commenators have too small a conception of "healthcare system." If reducing gun fatalities, lead in paint, air, and soil, and obesity, results in better healthcare outcomes, we should do it! And this could be done in a "libertarian" friendly way-increase taxes on consumption, reduce taxes on labor or capital (Sweden has done something like this, by taxing consumption way more than the US, but not taxing primary residences.) If automating driving could save us 12 9/11 attacks a year in fatalities and countless more injuries, we should include that in our health system....
-I think Michael O'Hare over at samefacts.com pointed out that the WHO found that the US accounts for 50% of medical research. This makes intuitive sense, since we are 25% of world GDP, with probably the other 30-40% of GDP of medical research being taken up OECD countries. Developing countries have more pressing priorities than trying moon-shots to cure cancer...
-Only 1% of healthcare costs can be related to ligitation. It is not a huge cost driver. Texas, Michigan, and a bunch of states reduced medical malpractice costs a decade ago and, to my knowledge, really did not bend the healthcare cost-curve.
-The Consulting Group McKinsey did a study 5-8 years ago about US healthcare costs. They found that the enviornmental "cheeseburgers and ice cream" of high US healthcare costs would only reduce healthcare by 1% of GDP. Not small potatoes or worth doing, but minor. They found that 3-4% GDP of US healthcare costs was due to the large amount of insurance companies we have. All the money chasing money, in other words...
Sorry for the soapbox but I hope I gave you some food for thought!
Frank
they found that the ukranian's are doing the same with less than five billion dollars a year.....well they have more fatalities but ....is a war raging on
DeleteAfter seeing your post I read that article first and then came to see your reply as it is the right thing to do in such cases of one replying to someone else for the obvious reason that was proven here. Suffice to say I was predictably disappointed.
ReplyDeleteThe most interesting point and main point of what is really the problem in his view is employer insurance.
Which you neglect to focus upon entirely, probably because you found the other points weaker and you prefer partisan attacking and proving your side right (both in your head and to others) facilitated by selecting quoting to truth seeking.
"Anyway, I do think Cliff's points are important. "
ReplyDeleteThat makes me think a lot less of you. Cliff is full of shit, and that was obvious as soon as he said that excluding murders and crashes moves us to #1. Unless you've got a perverse desire to wade through paragraphs of conservative swill, there's no point in continuing, this troll cannot even do arithmetic.
Dear Dr Noah:
ReplyDeleterespectfully, may I suggest that this country *really* needs a serious thougthfull person to take this on, it is a full time job
for instance, how does one count things like maternity leave in healthcare ?
certainly, other countries spend more, at least directly; intuitively, one would think that maternity leave is healthy...
another point, if you work physical labor job, and become injured, that injury can grow into something bad if you can't get a day or two off.
maybe other countries do a better job here ?
anyways, thanks
as an analog, there was a paper that ~ 50% of personal bankruptcys were medical related, pushback from the right, then pushback from the original authors, who, I think, had the best of it
Figuring out an apples to apples accounting of health care is quite a chore and not rigorously pursued in many studies. One example: health care personnel in the United States frequently carry large - even exceptionally large - debt related to their direct medical training. These debts get serviced out of the fees and salaries they charge and earn. This same category of medical education debt pretty much does not exist in many countries reporting lower health care spending. But those costs absolutely exist, but simply are accounted for as education not health care. That is a fair accounting as it goes, but to push a good part of this expense over to a nation's health care budget and the gap closes. The treatment of real property taxes can be completely different also. Your local out-patient surgery center may be paying full local property taxes in many places in the United States, while the equivalent in many countries would be exempt. Of course the rest of the tax base carries an increased load to make up for it, so put that into the health care category. Even construction costs of hospitals where the billboard in front says "Ministry of Health" you will often find that large chunks of the project budget may be coming from other sources not aggregated into health care costs. I do not challenge the accounting per se - if it is good with the accounting standards it is not bad accounting, just that if you accounted for the same laundry list that goes into US health care costs the gaps close down.
ReplyDeleteDOCCS services include various premier aesthetics such as laser fat loss, massage therapy and botox.This revolutionary method provides results without the dangers associated with surgery.
ReplyDeleteurgent care open 24 hours